When the Expected is Made to Sound Terrifying
by John Duffy
Alpha’s and Betas and Deltas, oh my! That’s right baby, variants of SARS-CoV-2 abound, and they’re coming to get’chya! If you pay attention to reporting on COVID19, you will have seen that especially starting in winter of 2020, the first winter of the COVID19 pandemic in the northern hemisphere, talk of scary new variants often dominates the conversation. Now, the first reporting I can recall on a SARS-CoV-2 variant was actually published in Scientific American back in July of 2020. The article was titled, “Second Coronavirus Strain May Be More Infectious—but Some Scientists Are Skeptical.” But before we dig into what the article says, let’s take a close look at the title. Notice anything? It doesn’t use the word “variant,” it uses the word “strain.” Are strains and variants the same thing when it comes to viral taxonomy? No, they are not.
The following text was written by Vincent Racaniello, who is a Higgins Professor in the Department of Microbiology and Immunology at Columbia University, for his blog post, Understanding virus isolates, variants, and strains
“A virus variant is an isolate whose genome sequence differs from that of a reference virus. No inference is made about whether the change in genome sequence causes any change in the phenotype of the virus. The meaning of variant has become clouded in the era of whole viral genome sequencing, because nearly every isolate may have a slightly different genome sequence. Such is the case for SARS-CoV-2: nearly every sequence from a different person is slightly different. Up until the end of 2020, any SARS-CoV-2 sequences from any two individuals differed by about ten nucleotide changes out of 30,000. They are all variants…
A virus strain is a variant that possesses unique and stable phenotypic characteristics. Such characteristics can only be ascertained by the results of experiments done in the laboratory…The name strain is not easily earned: certainly it cannot simply be given by journalists…No such designation of strain has been given more than once to SARS-CoV-2: there is one, and only one strain of this virus.”
So right off the gun, Scientific American was using improper verbiage in it’s title. They should have known this because the article is about a paper that was published in the journal Cell, which states in the bullet points right at the top:
“A SARS-CoV-2 variant with Spike G614 has replaced D614 as the dominant pandemic form” [emphasis mine]
Maybe it seems like I am nit picking, but this is Scientific American. It’s one thing to make blunders about the nuances of viral taxonomy in a publication that doesn’t have a regular science writer, but you’d think that Scientific American would have pretty much only science writers. Anyway, their article goes on to state that :
“The results showed that the G strain produced more of the virus in the human body than the D strain. But the former did not lead to a higher hospitalization rate, meaning it apparently did not cause more severe illnesses.”
And they concluded that:
“The paper by Korber’s team shows that antibodies from people who had been infected with SARS-CoV-2 fight against both strains.”
So why the hell do variants matter, especially if Dr. Racaniello is right and almost every single infection creates a variant by technical definition? What we should be concerned about is a virus that is more harmful/deadly (virulence), or that evades existing treatment or prevention protocols. However, if you look at most media reporting, talk of variants is usually couched in infectiousness, or what percentage of current cases are of a particular variant.
This was published by the BBC on June 24th, 2021
“…EU health officials said the [Delta] variant would account for 90% of the bloc’s cases by late August.
The spread could disrupt plans for lifting restrictions during the summer.
The Alpha variant, first discovered in the UK, hit Europe hard early this year and Delta, now dominant in the UK, is thought 40%-60% more transmissible.
Delta, first identified in India, now accounts for almost all new infections in the UK.
The UK is not on the EU’s list of safe countries, due to the spread of Delta, but that list is not binding on member states.
The UK is not safe! The Delta variant accounts for almost all new infections! It’s more transmissible! OK, but what are the results of this virus accounting for most new cases? Are more people dying? Are more people ravaged for life with scarred lungs? Are people turning blue and growing extra fingers? What?! Tell me
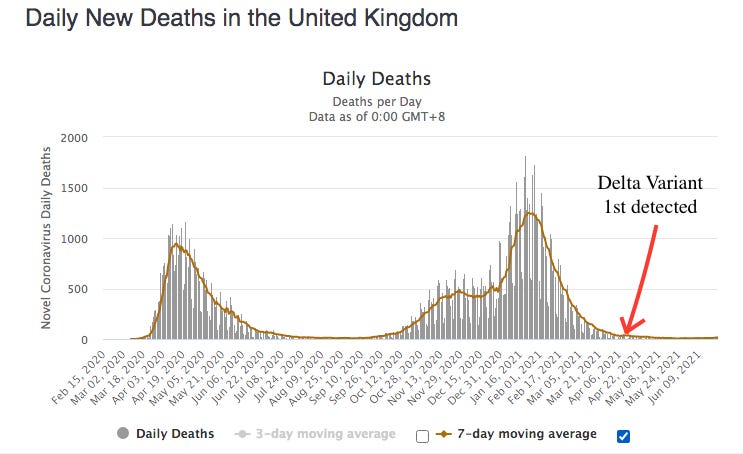
According to this article in Nature, the Delta variant was first discovered in the UK in mid April. Looking at the daily deaths in the UK since that time, it looks as though they only continued the downward trend they were already on. So why such concern? In fact, over the last year and a half, there has been a prevailing attitude in the media that variants were a terrifying reality that could at any moment, drastically alter the the trajectory of pandemic. There have been oodles of stories and blood curdling headlines about the UK variant, the South Africa Variant, the Brazil Variant, the India Variant, and so on and so on. We could never “let our guard down,” because these variants were unpredictable, novel versions of a novel virus, and nothing that we had learned in the previous months could be trusted. And now President Joe Biden is tweeting that the India Variant, aka B1617.2, aka the Delta variant is both more contagious and more deadly:
This notion that the Delta variant is more contagious and simultaneously more deadly would seem to run counter to common sense understanding of how a lot of viruses work. Viruses are not conscious entities trying to assassinate their hosts. Viruses operate on a biological imperative to self replicate, and they often achieve this best when they don’t kill their hosts. With many viruses, we see what has been dubbed the “law of declining virulence.” There are some who argue that this “law” doesn’t always apply, in that as long as a virus can replicate and spread before killing it’s host, it has achieved its goal, but again, looking at deaths, is that what we seem to be witnessing?
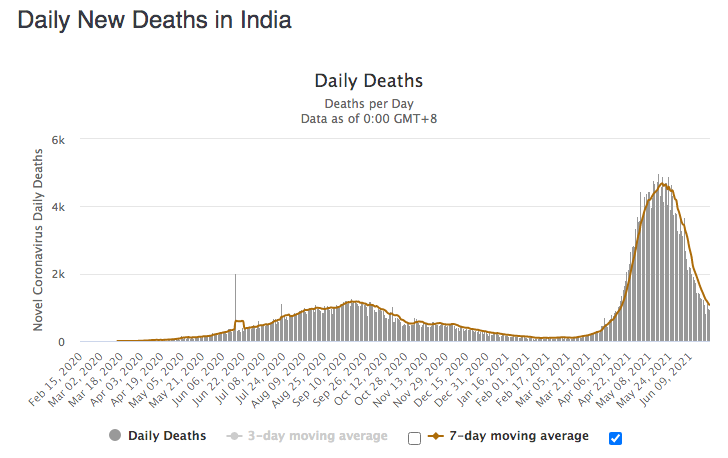
Looking at India where the Delta variant is thought to have first originated, we see a spike in spring deaths that has fallen as quickly as it has risen in a country that never really had a spike prior. (India was always seen as a head scratching anomaly up to this point, with such a large population, and with so many of those people living in poverty and squalor). India has nearly 1.4 billion people, and thus far has had just shy of 400,000 deaths from COVID19. If these numbers are accurate, that’s 282 deaths per million people, or .02% of the population. Compare that to the US’s 1,858 deaths per million, Belgium’s 2,161 per million, or Peru’s 5,724 per million. Sure, some will argue that India didn’t count right, or that tertiary deaths from lack of care drive up their totals, but those deaths do not give us a clear picture of the virulence of the delta variant and whether or not it is going against type and spreading more effectively while also killing more efficiently. Again, as of this writing, the spike in India seems to be over.
There has been a media trend across the course of the pandemic to highlight a variant or a country currently experiencing a spike in cases and deaths, and then to just move on when it turns out that variant didn’t end up actually having more virulence or when that country’s case and death numbers flattened. Here was a headline from May 2021:
As COVID-19 Rages in India, Scientist Warns Further Waves ‘Inevitable’
Look, I’m not a make believe virologist. The best I can do is read what’s out there, maybe talk to some virologists, and then write what I find. My overall concern, at the end of the day, is media, and how we as the public are spoken to. From what I have seen, too often during the pandemic the most explosive, the most terror inducing language has been used to garner attention, and this has resulted in populations that drastically overestimate the threat of COVID-19. According to Brookings:
“…the average American dramatically overestimates the share of COVID-19 deaths from people aged 24 and younger, putting it around 8%, when in fact it was 0.1% through August and has remained close to that level since. Meanwhile the elderly, those 65 and older, had accounted for 81% of deaths at the time of the survey (and 79% through November). Democrats were further off than Republicans and more likely to overstate the risks to young people, even after accounting for age, race, gender, geographic, and educational differences.”
The Brookings data goes on to highlight as well, that people, especially democrats, drastically overestimated how many people who came down with COVID-19 had to go to the hospital – which was between 1% and 5%, not the 50% that almost half of democrats polled responded.
Should we be scared of variants? As of right now, my humble answer would be no, and to explain why I will again refer to the writing of Dr. Vincent Racaniello:
“The observation that variants of concern are less effectively neutralized by antibodies against ancestral strains have led to predictions of vaccine failure and doom. This outlook is incorrect: amino acid changes in the spike protein of SARS-CoV-2 variants of concern do not impact T cell reactivity and are not likely to affect the ability of T cells to clear infection. This conclusion has been emphasized by the results of another study which show that SARS-CoV-2 variants of concern partially escape humoral but not T-cell responses in COVID-19 convalescent donors and vaccinees.”
So keep this all in mind when the Togo variant, or the Iceland Variant, or the East St. Louis Variant come roaring into the headlines with associated experts predicting “doom this time.”
Excellent article. Thanks for the clarification of variants and strains… so, no new strains, only variants.
The reason that every sample tested shows up as a slightly different “variant” has to do with the way they come up with gene sequencing. DO NOT IMAGINE (!!!) that they somehow isolate a virus and then check out all its imaginary 30,000 nucleotides in some sort of empirical fashion. No. They take a sample, culture it, never purify, reduce it and then “assemble” a gene sequence by piecing a bunch of tiny particle sequences together from an unknown sludge of material that has never been shown to be part of a virus, using a computer program designed to do just that. THE REASON that one “variant” looks similar to another is that the only way that can come up with such an outlandish sequence is by basing it on a previous sequence… thus the SARS-COV-2 sequence is BASED ON SARS, MERS and other such sequences. None of these viruses has ever been isolated and studied empirically. EVER. To get an idea how all this works, please check out “Covid-19 Myths” video on Andrew Kaufman’s website. The whole process is absolutely ludicrous.
I was going to write about that but luckily I read your comment first, so I don’t need to write.
How it works, is simple: Using an easily manipulated lab tool PCR, one can have the final result one desires.
Then use the PCR kit to pretend that good old PNEUMONIA is a new thing and just start printing PCR “COVID-19” labels, and voilà a PCR PANDEMIC is born.
Hello…
Special congratulations to the author of the Cartoon. I always enjoy to see that other fellow modern slaves know Numerology that the Secular Ruling Families & Billionaires use.
C’mon we shouldn’t even be scared of mythical database/software engineered RNA “SARS-CoV-2”.
PNEUMONIA is NOT NEW, it kills every year millions of uman animals so it is the perfect REAL disease to be used when one wants to pretend that a “deadly pandemic” exists!